The Contribution of Selected Urinary Solutes to the Determination of Urinary Osmolality in Guatemalan Preschool Children Consuming a Common Menu Offering

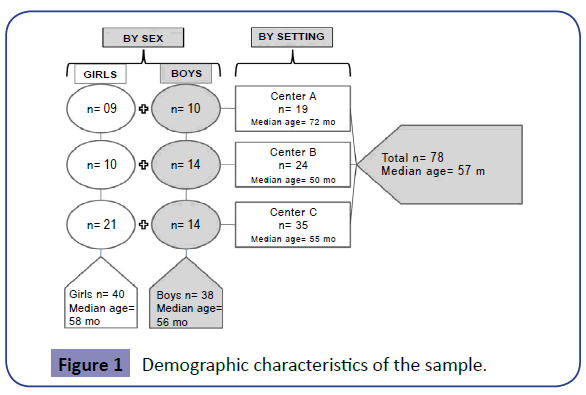
Although water is the most abundant and most vital of all human nutrients, hydration is among the most ignored aspects of human nutrition. Many different solutes are eliminated by the kidneys in the urine flow, potentially contributing to the osmotic charge of this body fluid and acting as determinants of the urinary osmolality [Uosm]. To measure urine osmolality concurrently with urea, uric acid, calcium, magnesium, potassium, sodium and inorganic phosphorus in a 24 h sample and to determine the patterns of their mutual interactions towards assessing the primary determinants of Uosm. Seventy-eight children from 2 to 7 years old, 40 girls and 38 boys, with median age of 57 mo underwent 24 h urine collections, with an aliquot separated for measuring urine osmolality by freezing-point-depression osmometry and solute concentrations by various analytical chemistry techniques. Spearman correlations and multiple regression models were run to assess interactions. Backward-elimination multiple-regression models found that the urinary concentrations of inorganic phosphorus, urea, sodium, potassium and magnesium explained 95.1% of the variance in Uosm among the seven analytes quantified; calcium and uric acid made negligible contribution. The analyses allowed us to confirm the determinant roles of urea and the principal electrolytes, sodium and potassium, for urine osmolality and to appreciate coordination in the collateral collinear associations with other excreted solutes.
The volume of water from all sources, including beverages, water in recipes, intrinsic food moisture and metabolic water from energy-substrate oxidation, is one determinant of hydration status. The minute-by-minute retention or excretion of this water is governed, in part, by renal regulatory mechanisms that filter the circulating stream of plasma containing a host of small, electrically-charged and neutral uncharged constituents to be excreted in the urine. These atomic and molecular species, themselves, initially originate in the diet. In some instances, they can be turned over and excreted on the same day of ingestion, as in the case of sodium [Na], potassium [K] and chloride. Alternatively, they may have been incorporated for various time intervals in bone or muscle, as with calcium [Ca], magnesium [Mg] and phosphorus [Pi], or in any soft tissue such as muscle or visceral organs, as with the amino acid-derived nitrogen, excreted as urea. Furthermore, the nucleic acids in the plant and animal cells in the diet and from endogenous sources of human tissues yield uric acid, eliminated by the kidneys in the urine flow. As ions and minute molecules in the urine, these− and many other solutes−contribute to the osmotic potential of this body fluid and constitute the basis for the Uosm. For young children then, the daily water balance plus the dietary food selection and the turnover of growing tissues would interact, in combination, to determine the osmolality as measured in urine.
We recognize a series of strengths and limitations in the present study. A major strength is that it addresses the age-group of young children, a population segment relatively ignored in the existing literature. Furthermore, it brings together the skilled analysis with modern osmolality equipment with an effort at quantitative collection of urine and the concurrent analysis of seven important solutes in human urine derived from the diet, endogenous tissue breakdown or both. Our children are offered a common and controlled dietary menu of both foods and beverage within the institutional center-day, which might theoretically narrow the sample-wide variance. At the same time, the latter constitutes a contextual limitation, as that the study series is a convenience sample of children with unique dietary long-term homogeneity, generalization to the population at large would not be justified. Furthermore, although the intention was to collect quantitative 24 h urine excretion on all collection occasions, an internal indicator suggests that this was accomplished only in a slight majority of instances. In conclusion, a situation in which a defined offering of an institutional menu and efforts at 24 h urinary collections converged in the study of systematic Uosm measurement; this has facilitated our gaining insights into the relationship of urinary excretion of selected solutes in the context of their relationship to Uosm, which is a proxy indicator for human hydration state. The most striking features overall in this group of relatively well hydrated preschool children is the inter-individual variation in excretion of the specific species analyzed. The analyses allowed us to confirm the determinant roles in Uosm of urea and the principal electrolytes, Na and K and to appreciate a harmony in the collateral collinear associations with other excreted solutes.
For more info kindly visit our Journal: https://clinical-nutrition.imedpub.com/
Best Regards,
Joseph Kent
Journal Manager
Journal of Clinical Nutrition & Dietetics